A 10-Step Occlusion Checklist for the Hygiene Room
By Donna Stenberg on June 7, 2016 | commentsThe hygiene visit is a cornerstone in a busy general dental practice. It is where patients not only receive education and treatment, but also receive an examination of the oral soft tissue structures, the dentition status and the periodontal health. Each status is documented in detail and a history is created so it can be followed over time. Often an initial diagnosis and additional treatment recommendations also begin in the hygiene room appointment.
To achieve all of that in one very full appointment requires streamlined systems to maximize the productivity. The periodontal and dentition documentation are well established for the hygiene appointment. Probing depths and bleeding indexes, tooth numbers and restorative tracking are ingrained early in education and in clinical practice. What is less systematized is tracking the developing occlusion.
An important aspect of treatment decisions is using the patient history to understand the progress or severity of problems, using that to guide recommendations. Equally valuable is monitoring the patterns that are expressed in dental, jaw and facial development. Using a checklist system will help to identify issues we don’t always see if we don’t look for them. When it comes time to make a treatment referral it is beneficial to know when the cross bite developed. Or that the open bite has reduced with each six-month exam. Your treatment decisions may alter if the airway has not improved for the last two visits. Or if the midline is now off by another millimeter. With good documentation you are able to inform patients and families of issues that may need additional evaluation in the future. It will not be a surprise when you make a referral for an issue that you have already identified for them.
Using this “top 10” checklist can organize your documentation into an easy system to follow and update with future visits. As with any new system, it will take several times to become efficient, but once practiced can be completed in a few minutes.
Some considerations are listed below for each measurement.
The Checklist
1. Overbite: A deep bite can be associated with incisor wear. An open bite may have a habit or airway component.


2. Overjet: An excess can indicate a developing Class II growth pattern, dental protrusion or narrow arch width.

3. Upper midline: With lips at rest and slightly apart, midline should be within the philtrum (cupids bow). Off-center midline can indicate crowding, a developing crossbite with palatal incisor eruption, or early primary tooth loss.

4. Lower midline: This can be an indication of a lower jaw growth asymmetry, crossbite, early loss of primary teeth or crowding

5. Cross bite: Posterior can indicate a lower jaw growth asymmetry or a narrow upper arch; anterior can indicate a developing Class III pattern or crowding with palatal eruption and a functional shift.

6. Crowding: Mild is in the range of up to 4 mm of crowding, moderate range 6-8 mm or more, and severe is 8 mm of crowding or more.

7. Palate width: 36-38 mm is the range of normal with normal range tooth size. Less than 31 mm and there is a high risk for severe crowding.

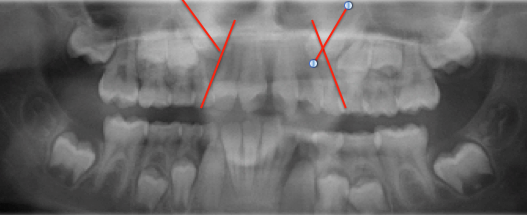
8. Canine position: Screening for canine position by age 10 can increase the potential to successfully improve an ectopic (impacted) eruption pathway. Comparing the angle of the canine crown to the distal contour of the lateral incisor from crown to root tip can indicate if active treatment is indicated.
9. Missing teeth: Noting this early can assist with awareness and planning discussions for replacement.

10. Airway: Easy breathing through the nose with lips resting together is ideal. Stuffiness, tonsils and adenoids, allergies, lip strain and snoring can be indicators for referral to an ENT for evaluation.

(Click this link for more orthodontic articles by Dr. Donna Stenberg.)
Donna J. Stenberg D.D.S., M.S., P.A., Spear Visiting Faculty and Contributing Author. djstenbergdds@gmail.com
References
McNamara JA, Brudon WL, Kokich VG. Orthodontics and Dentofacial Orthopedics. Ann Arbor, MI: Needham Press; 2001.
Schindel RH, Sheinis MR. Prediction of maxillary lateral-incisor root resorption using sector analysis of potentially impacted canines. Journal of Clinical Orthodontics. 2013;47(8):490-493.