Lip, Tooth, Ridge Classification Part 2: Risk Assessment
By Ricardo Mitrani on August 12, 2017 | commentsThe LTR classification integrates two fundamental processes. The first consists of carrying out a risk assessment in two different areas:

- Esthetic risk: In order to evaluate such risk, we have to incorporate the relevance of lip dynamics into our decision process. There are two different ways this could play out:

a) High Esthetic Risk (HER) lip mobility that exposes the transition line between the prosthesis and the ridge.
b) Low Esthetic Risk (LER) lip mobility that does not expose such a transition line.
- Structural risk: It shouldn’t come as a surprise that space availability plays a huge role in any given prosthetic design. Inadequate space may lead to biomechanical failure. For this matter, we should consider two different scenarios:
a) High Structural Risk (HSR): Such risk is present when inadequate space for componentry and materials is available.
b) Low Structural Risk (LSR): Patients present appropriate space.
The second fundamental process is categorizing the patient into four possible clinical scenarios based on the deficiency of hard and soft tissue between the ridge and the teeth in a vertical aspect and between the ridge and lip in a horizontal aspect. We’ll divide these scenarios into four different classes.
Class I Esthetic Risk
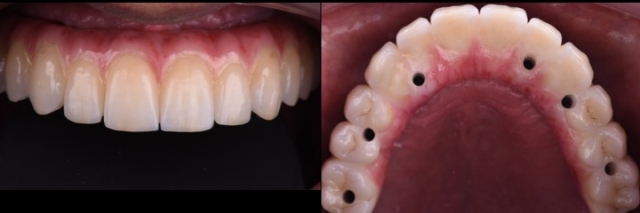
This clinical condition poses the ideal scenario for a “conventional implant-supported crown and bridge prosthesis.” A Class I patient has minimal tissue deficiency, which means no gingival prosthetic material is needed.
This implant-supported prosthesis is commonly fabricated utilizing metal-ceramics, though zirconia can also be used. Keep in mind that adequate connector sizes are critical, depending on the type of retention selected, this typically means at least 7 to 10 mm of vertical prosthetic space. The vertical prosthetic space is the space from the platform of a bone-level implant to the occlusal surface of the restoration.
Of course, there are some other factors we’ll need to evaluate. In maxillary edentulous situations, the healing pattern that occurs after multiple tooth extractions leads to a flat ridge configuration. The development of a scalloped soft tissue contour is not predictable, and the use of bone and soft tissue augmentation techniques will provide sub-optimal outcomes in the interproximal areas. Therefore, achieving a harmonious relationship between the tooth structure and the underlying soft tissue will require creating an illusion through a prosthetic compensation, such as long contact areas and/or the ceramic characterization of the gingival embrasures.
The management of interdental papillae still poses a challenge for Class I-LER. This is because 87 percent of dentate patients presenting a low lip line still feature interdental papillae on exaggerated smile.
On the other hand, the Class I-HER presents an increased esthetic risk due to greater soft tissue display. In these cases, we need to execute adequate soft-tissue “grooming” and may need to use interdental gingival prosthetic material in certain situations.



Class II Esthetic/Structural Risk
This clinical condition consists of a larger vertical deficiency between the cervical margin of the proposed maxillary central incisor and the alveolar ridge.
This situation requires pink colored prosthetic material (ceramic, composite or acrylic). We can fabricate this type of prosthesis using metal-ceramics, zirconia-ceramics or metal-acrylic. The metal-ceramics and zirconia-ceramics designs will require an average of 8 to 12 mm, while the metal-acrylic requires 13 to 15 mm in the posterior area.


A Class II-HER presents a high esthetic risk because the junction between the prosthesis and the residual ridge needs to be hidden under the upper lip position upon exaggerated smile. For this reason, precise pre-surgical planning is absolutely critical, and must include a surgical template that will ensure adequate bone reduction is performed to meet the aforementioned goals.
If anatomical structures limit the removal of bone for prosthetic/esthetic needs, we need to consider an alternative design in order to bypass the anatomical limitation and/or lack of sufficient bone for implant placement. Examples of this alternative design could be distally tilted implants, alternative implant distribution or the use of zygomatic implants.
Stay tuned for the last article in this series, which will cover Class III and IV clinical scenarios.
(Click this link for more dentistry articles by Dr. Ricardo Mitrani.)
Ricardo Mitrani, D.D.S., M.S.D., Spear Faculty and Contributing Author
References:
- Stein RS. Pontic-residual ridge relationship: a research report. J Prosthet Dent. 1966 Mar-Apr;16(2):251-85.
- Goldstein RE. Esthetics in Dentistry. Philadelphia: J.B. Lippincott, 1976:425-455.
- Hochman MN, Chu SJ, Tarnow DP. Maxillary anterior papilla display during smiling: a clinical study of the interdental smile line. Int J Periodontics Restorative Dent. 2012 Aug;32(4):375-83.
- Dong JK, Jin TH, Cho HW, et al. The esthetics of a smile: a review of some recent studies. Int J Prosthodont. 1999;12(1):9-19.