 This 8-year-old patient presented to my office in late October of 2005, having fallen from her bicycle earlier in the day. In addition to the small lacerations and contusions, #8 and #9 had sustained fractures that made their restorative prognosis hopeless (Fig. 1).
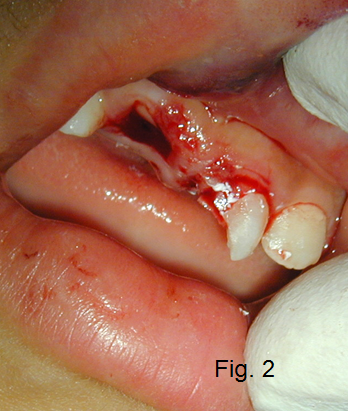
This 8-year-old patient presented to my office in late October of 2005, having fallen from her bicycle earlier in the day. In addition to the small lacerations and contusions, #8 and #9 had sustained fractures that made their restorative prognosis hopeless (Fig. 1).Extracting these teeth on an 8-year-old would leave an alveolar ridge defect of significant magnitude. This would make future tooth replacement problematic whether we used implants or a conventional fixed partial denture. I recommended banking the remaining roots to preserve the alveolar ridge (Fig. 2).
The teeth were isolated, which required packing cord, clamping gingival tissue and removing coronal pulp from the root. White mineral trioxide aggregate (ProRoot MTA) was placed over the remaining pulp tissue. At the time of treatment, it was reported that the MTA would not set without a source of moisture, so it was covered with a moist cotton pellet and then sealed in place with bonded Corepaste.
The patient returned mid-November of 2005; the Corepaste and the cotton pellet were removed and the set MTA sealed only with bonded Corepaste. A surgical flap was subsequently reflected, the remaining tooth structure beveled even with the alveolar ridge and the flap sutured closed.
 The patient was sent back to the referring pedodontist and an acrylic removable partial denture was fabricated (Fig. 3). The patient was followed and the site healed without incident. No sign of apical periodontitis had become evident and the remaining pulp tissue reacted as expected, continuing to produce dentin resulting in pulp canal obliteration.
The patient was sent back to the referring pedodontist and an acrylic removable partial denture was fabricated (Fig. 3). The patient was followed and the site healed without incident. No sign of apical periodontitis had become evident and the remaining pulp tissue reacted as expected, continuing to produce dentin resulting in pulp canal obliteration.In my next article, I will go over her five year follow up, as well as her nine year.
Glen E. Doyon, DMD, Spear Contributing Author [ www.CMSEndo.com ]
Comments
June 12th, 2014
June 19th, 2014
June 19th, 2014
June 20th, 2014
June 20th, 2014
September 25th, 2014