Try Before You Buy: Evaluating Indirect Restorative Impression Materials
By Jeffrey Bonk on June 3, 2019 |Are your restorative impressions accurate?
Are you impressed with your restorative impression material?
Buyers beware! Are all polyvinyl impression materials equal?
These are all questions dentists have when it comes to final impressions for definitive indirect restorative dentistry. Accuracy, repeatability and predictability are the objectives for impression materials in clinical practice. This article will provide some insight into impression materials selection and evaluation.
Polyvinyl siloxane impression materials are widely used in restorative dentistry for obtaining final impression for indirect restorations. Digital impressions are on the rise due to advances in CAD/CAM systems. Efficiency and patient acceptance are primary driving forces behind the digital dentistry explosion. Both techniques can provide acceptable results, but traditional analog type impressions remain the gold standard for most restorative dentists.
Factors that influence impression accuracy include proper material handling, the clinicians experience and skill, impression technique, working time, number of restorations to be impressed and patient compliance. Additionally, finish line location, preparation smoothness, tissue management and moisture control influence the accuracy and relate to the success of final restoration outcome. The multitude of factors and considerations necessary for obtaining an acceptable final impression are daunting.
When we clinicians find an impression material and technique that provides repeatable and predictable outcomes, it is rare to contemplate and accept a change of material. We are not only creatures of habit, but also our staff and systems are smooth running machines that continually provide predictability and success with the materials and techniques to which we are accustomed. Life is good when the patient's impression appointment runs smoothly and indirect restorations fit.
But! There are always the nagging questions:
“Is there a newer, better and more accurate material for obtaining indirect impressions?”
“Am I lagging behind my peers, because I am not using the newest and the best material available?”
“I don’t want to be ‘old-school’ just because of habit!”
“What am I supposed to do?”
The answer: Contact your friendly materials representative and obtain some samples of the “greatest and best” impression material on the market. While I am being facetious, our dental product representatives are very knowledgeable and helpful when contemplating changes of materials, products or techniques.
I personally rely on my sales representatives for a tremendous amount of information. A good sales representative knows product and has a handle on what works and what doesn't. They know your practice and they are aware of the type and quality of dentistry that is provided from your office.
The key factor in changing materials is that we self-assess how the new material works in our hands. Does the change create better outcomes? Will using this material improve final fit and marginal integrity? Personal assessment is key. This self-assessment process is comparable to taking a Spear Workshop, which introduces attendees to new ideas, concepts and techniques over the course of three hands-on days at the Spear Campus in Scottsdale, Arizona. The information presented must be integrated and tried by the workshop participant in their practice to determine whether the outcomes are better.
You should not rely solely on the recommendation of the presenter. If the outcome improves after integrating and evaluating the new concepts or techniques, then a permanent change can be implemented. A change in impression material is the same. Changing impression materials must include self-evaluation, rather than reliance verbal recommendation.
While seemingly obvious, many dentists have storerooms full of products purchased on recommendation that did not provide promised results. Do not fall into a trap of purchasing material solely on verbal recommendations. Use it, abuse it and evaluate the results in comparison to your existing materials and techniques.
Many factors relate to final fit and accuracy of the final indirect restoration.
There are many impression materials available on the market: polyethers, silicones, hydrocolloids and various polyvinyl siloxanes, to name a few. Polyvinyl siloxane is the most commonly used impression material. It has high accuracy, good dimensional stability, good elastic properties, high tear strength, short working and setting times and excellent recovery from deformation upon removal. Additionally, it is highly stable over time and has minimal shrinkage, so impressions may be poured days later. These properties are well documented in the literature.
There are two techniques used when working with polyvinyl impression materials. Either a one stage or two-stage technique is applied. One stage refers to the ‘wash’, or lighter body material being applied to the tooth preparation with the heavy body or unset putty placed in the tray and seated over the light body material. The more viscous the light body material, the less filler content it has. Less filler content relates to ultimate dimensional stability. This is referred to as the “shear thinning effect.”
The two-stage technique refers to the initial putty impression being made prior to tooth preparation and allowed to set. Once the tooth is prepared, the light body material is utilized as a wash to reline the putty. Hung, et.al., reported that a single stage is more accurate due to dimensional alterations that can occur between the set material and the added light body wash. The literature is complete with multiple scientific data on materials and testing criteria. Technique and process are crucial to the ultimate accuracy. Regardless of the technique utilized and the recommendation of the manufacturer, the clinical dentist must analyze and evaluate the final model.
Recently, I was introduced to a polyvinyl impression material that was different than what I had been traditionally using in my practice for many years. This introduction came my product representative whom I trust immensely. The recommendation was that this material was superior to the product I have been using successfully. While I was happy with the present material, I was curious as to how the new material would perform (I am specifically not providing product or representative names).
My point in this article is that self-evaluation is key to the determination of material change. As much as the product may be touted as “better than” or “more accurate than,” individual assessment is the final determinant. Clinical performance rules!
I have provided some images that represent my findings and observations of the single-stage impression technique utilized in this evaluation. My technique, traditionally, is a light body syringe material followed by a heavy body material loaded into a full arch custom tray. I use a two-cord technique as means of tissue retraction. The images represent tooth preparations for ceramic (EMax) onlays.
Image 1. (Traditional polyvinyl impression)
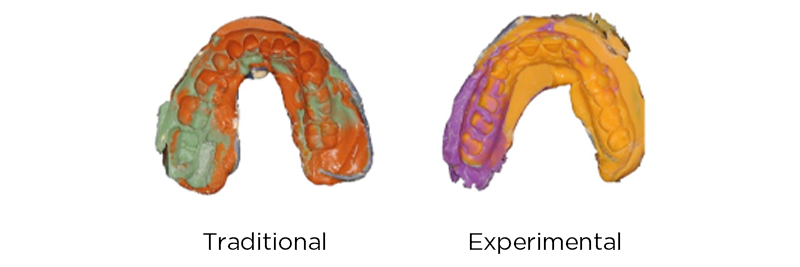
This image shows the traditional impression material utilized in my office for many years. There is good contrast between prepared and unprepared tooth. Additionally, the material color difference aides in improved visualization of preparation margins.
Image 2. (Testing material polyvinyl impression)

This impression material does not provide easy delineation between prepared tooth and unprepared tooth. The material color similarities do not provide adequate contrast for margin evaluation. Generally, my dental laboratory double pours the polyvinyl impressions for final indirect restorations. The first pour becomes the pinned die model utilized for definitive margins with a wax and press restoration fabrication technique. A second pour of the polyvinyl impression is utilized as a solid, unpinned model to check contacts and occlusion. Both models are face bow mounted on semi-adjustable articulators.
Image 3. (First pour die model- traditional impression material)

This is a close-up perspective of the onlay preparation first pour pinned model. This model was fabricated from the traditional polyvinyl siloxane that has been used in my office for many years. The preparation margins are clear and sharp.
Image 4. (First pour die model- testing impression material)

The stone models produced form the first pour of the testing material provides good, crisp margins that can predictably be utilized for final ceramic fabrication. It is challenging to delineate between the traditional model and the testing model.
Image 5. (Second pour- traditional impression material)

The marginal accuracy of the second pour of the traditional material shows no change from the stone model produced from the first pour. The stability of the impression material is verified by the crisp and accurate margins produced.
Image 6. (Second pour testing material- solid model)
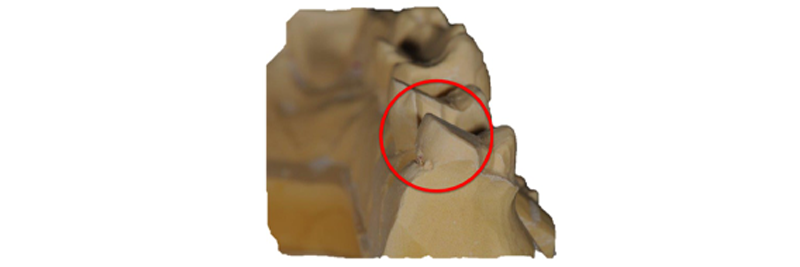
This model shows a loss of marginal sharpness and crispness. There is a “rounding” of the stone margins. This inaccuracy would result in open margins and an unsatisfactory cement line. While the test material is supposed to withstand multiple pours, it appears that the outcome is substandard and unacceptable. The first pour model is typically utilized for restorative margin adaptation and refinement, though it is important to be able to check the restoration on an accurate second model to verify marginal integrity.
There are many factors related to accuracy of polyvinyl siloxane impressions and stone casts produced from them. Small changes in dimensional accuracy among polyvinyl siloxane materials can be attributed to variability in the matrix-filler ratio of the material. The various ratios can provide different levels of polymerization shrinkage and elastic recovery.
Setting expansion of die stone may also be a consideration in the observed inaccuracies between models. The type of die stone utilized, method of stone mixing and the use of surfactants during the stone pour may all affect the ultimate dimensional outcome of the model.
At this point, I am still evaluating an impression material change. I have spoken with my representative about my self-evaluation findings. He was very interested in the photos and documentation I have shared in this article. We are discussing alternative materials and are continuing trials. The bottom line when contemplating a change in impression material, or any other change of dental materials for that matter, is to utilize self-evaluation as a final determinant for change. If the material, technique and ultimate outcome are better, faster, and/or more accurate, then the change can be good.
Utilize your product sales representatives as sources of information. They are a good resource. But, in the end, “try before you buy” and be critical about the performance and the outcome before a permanent change is initiated.
Jeffrey Bonk, D.D.S., is a member of Spear Resident Faculty.
References:
Vinyl polyvinyl siloxane impression materials: a status report. Council on Dental Materials, Instruments, and Equipment. J Am Dent Assoc. 1990;120:595-596, 598, 600..
Hung SH, Purk JH, Tira DE, Eick JD. Accuracy of one-step versus two-step putty wash addition silicone impression technique. J Prosthet Dent. 1992;67:583-589.
Dogan, S. et.al., Clinical efficacy of polyvinyl siloxane impression materials using the one-step two viscosity impression technique. JPD 2015, Vol. 114(2), pp.-217-222
Ho, W., Lin Seow, L., Musawi, A., Viscosity effects of polyvinyl siloxane impression materials on the accuracy of the stone die produced. J Clin Transl Res. 2018 Apr 12;4(1):70-74.