Corticotomy-facilitated Orthodontics and Goal-oriented Treatment Planning
By Rebecca Bockow on October 29, 2016 |Have you ever had a patient decline orthognathic surgery? Or a patient who needed orthodontics but did not pursue it because the projected treatment time was too long? Have you ever seen a patient with significant gingival recession who would also benefit from orthodontic treatment?
Thanks to new developments in interdisciplinary dentistry, we can now offer exciting and innovative treatment options for our patients.
Patients seeking orthodontic care may present with dental crowding and/or skeletal discrepancies. When the etiology for a malocclusion is skeletally-based, a patient's treatment options include either a combination of orthodontics and orthognathic surgery or orthodontic “camouflage” treatment, including extractions, interproximal reduction, and pushing teeth to the their biologic extremes. The biologic limits of orthodontic tooth movement are defined by the pre-treatment alveolar bone and the surrounding soft tissues. Moving teeth outside of the alveolus can result in bony dehiscences, fenestrations and gingival recession.
Corticotomy-facilitated orthodontics as a treatment alternative to orthognathic surgery
Traditionally, the only treatment option for patients requiring tooth movement beyond the scope of orthodontic camouflage was a combination of orthodontics and orthognathic surgery. Some patients decline orthognathic surgery due to fear, cost, lifestyle or underlying health issues. We now have an effective treatment option to offer borderline surgical orthodontic patients.
In implant dentistry, when the alveolar ridge is deficient to support the placement of an implant, we perform a localized bone graft, or a “guided bone regeneration.” The same principles can be applied to orthodontic tooth movement: If there is insufficient bone to support traditional tooth movement, we can now ask our surgical colleagues to graft the alveolus. Advantages to this procedure include greater breadth of tooth movements, potentially less gingival recession, greater long-term orthodontic stability1 and a faster total treatment time for the patient.2 Studies show that tooth movement can be twice as fast in the presence of a localized injury compared to traditional orthodontic tooth movement.3,4 If a patient declines orthognathic surgery, we can now expand the alveolar ridge and safely move teeth a greater distance in order to mask an underlying skeletal discrepancy.
Interdisciplinary treatment planning and case selection
Diagnosis and treatment planning from all team members is essential for a favorable treatment outcome. The ideal position of the teeth should be determined in three planes of space. The final restorative treatment plan may influence the ideal tooth position. Once the team knows the tooth movement goals, the surgeon and orthodontist assess whether or not the available bone can support such movement. If the answer is no, a localized bone augmentation is necessary in the direction of the proposed tooth movement. Brackets and wires are placed a few weeks to a few months prior to the surgery.
Immediately following bone augmentation, the teeth are rapidly moved into the grafted bone. The new bone heals around the teeth as they move into the new position, creating increased post-orthodontic tooth and soft-tissue stability
Case example
Initial presentation:
A 28-year-old female patient presented to the orthodontic clinic with a chief complaint of, “I don’t like my smile and my open bite.” Prior to her initial presentation, the patient declined all treatment options requiring a maxillary LeFort surgical procedure due to fear. (Figures 1-3)



Goals of treatment:
Treatment goals were planned around an ideally positioned maxillary central incisor in three planes of space. All idealized tooth movements, if performed with traditional orthodontics, would have pushed the tooth roots outside of the alveolar housing. Most of the large idealized tooth movements were isolated to the maxillary arch. (Figure 4)

Treatment plan and therapy:
The goals of tooth movement in the maxillary arch included transverse expansion and anterior protraction and extrusion. All proposed maxillary tooth movement was in the buccal direction. Therefore, only the buccal maxilla required segmental decortication and bone augmentation.
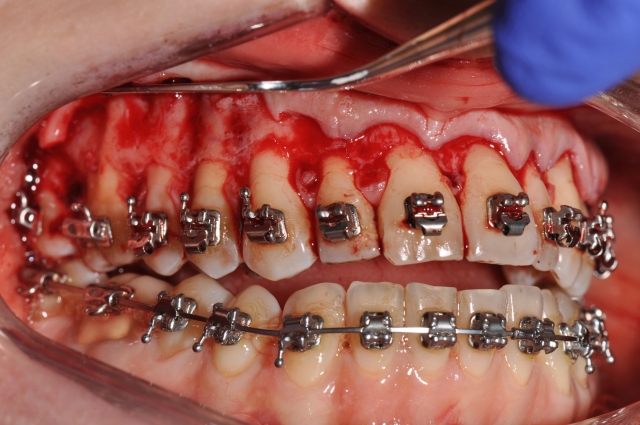
Large bodily tooth movements were initiated immediately following a selective alveolar corticotomy and bone augmentation procedure, allowing the alveolus and teeth to remodel to the desired new position during the period of high bone turnover and subsequent healing. Following leveling and aligning, a full thickness flap was reflected and alveolar corticotomies were performed along the buccal surfaces of the maxilla, spanning from second molar to second molar. (Figure 5) The alveolus was grafted with re-hydrated sterile particulate freeze-dried human bone allograft, and the flaps were repositioned and sutured to place. Healing was uneventful.
The patient was seen every two weeks in order to assess the treatment progress and to advance the orthodontic tooth movement. Large tooth movements occurred efficiently within the weeks following the surgery. (Figure 6)

The final finishing and detailing stages of the patient's treatment were completed within the same time frame as with any orthodontic case. (Figure 7)

Results:
Tooth movement goals as outlined in the original treatment plan were achieved (Figures 8 to 15).








Total treatment was completed in less than one year. The success seen in this case is not from the speed of orthodontics, but from the dramatic range of tooth movements achieved without orthognathic surgery and without adverse sequelae to the teeth and periodontium.
For this patient, only maxillary buccal bone grafting was utilized, minimizing the surgical intervention. Many patients are now being treated with a combination of both hard- and soft-tissue grafting materials, thus changing the tissue thickness, correcting recession defects and further preventing future recession. All teeth as well as occlusal and soft tissue changes remained stable at the patient's one-year retention visit.
Conclusions
Orthodontics combined with selective alveolar decortication and bone augmentation can lead to dramatic outcomes and, when appropriate, may be an alternative for borderline orthognathic surgical candidates. Clear treatment objectives, proper case selection, goal-oriented orthodontic mechanics, sequencing and timing all play a role in the successful outcomes of these cases.
Rebecca Bockow, D.D.S., M.S. www.SeattleSmileDesigns.com
References
- Rothe LE, Bollen AM, Little RM, Herring SW, Chaison JB, Chen CS, Hollender LG. Trabecular and cortical bone as risk factors for orthodontic relapse. Am J Orthod Dentofacial Orthop. 2006. Oct;130(4):476-84.
- Wilcko MT, Wilcko WM, Pulver JJ, Bissada NF, Bouquot JE. Accelerated Osteogenic Orthodontics Technique: A 1-Stage Surgically Facilitated Rapid Orthodontic Technique with Alveolar Augmentation. J Oral Maxillofac Surg. 67:2149-2159, 2009.
- Mostafa, YA, Fayed MM, Mehanni S, ElBokle NN, Heider AM. Comparison of corticotomy-facilitated vs standard tooth-movement techniques in dogs with minis crews as anchor units. Am J Orthod Dentofacial Orthop 2009; 136:570-7.
- McBride MD, Campbell PM, Opperman LA, Dechow PC, Buschang PH. How does the amount of surgical insult affect bone around moving teeth? Am J Orthod Dentofacial Orthop 2014;145:S92-9.