Esthetics
Treatment Decisions: To Remove or To Retain?
By Greggory Kinzer on March 4, 2015 | 0 comments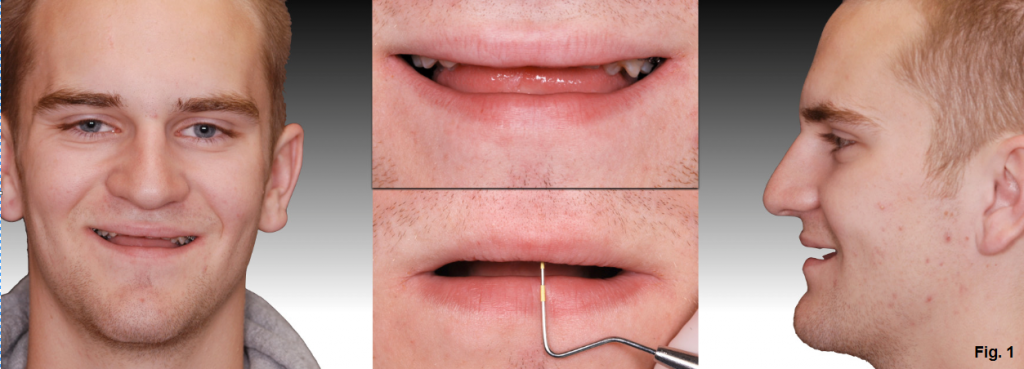 Imagine if this was your patient and he was presenting to your office for a second opinion on treatment. What would you? This 18-year-old patient presents with a lack of tooth display on the maxillary arch. (Fig. 1)
Imagine if this was your patient and he was presenting to your office for a second opinion on treatment. What would you? This 18-year-old patient presents with a lack of tooth display on the maxillary arch. (Fig. 1)He is congenitally missing his canines and has a Grade I+ of all of the maxillary incisors due to their excessive proclination and trauma from occlusion. Also note that there is essentially no root left on the left central incisor. (Fig. 2)
 The treatment plan that he currently has is to do a LeFort I to move the maxilla down and improve tooth display and extract the maxillary centrals and laterals (because of the excessive mobility and short root). When the patient stopped growing, the teeth would be replaced by augmenting the ridge with an iliac crest graft and placing implants. Now, ask yourself: what you would do?
The treatment plan that he currently has is to do a LeFort I to move the maxilla down and improve tooth display and extract the maxillary centrals and laterals (because of the excessive mobility and short root). When the patient stopped growing, the teeth would be replaced by augmenting the ridge with an iliac crest graft and placing implants. Now, ask yourself: what you would do?Are implants better than teeth? What about the short root on #9? How will that hold up over time? Is a resorbed root enough to necessitate the removal of a tooth?
 When I saw that patient, my thought was to retain the incisors and retract them thereby closing the edentulous canine sites and having the first premolars become the canines. Since the patient already required a Lefort procedure, why not advance the maxilla at the same time? This would allow the patient to keep his anterior teeth by correcting the anterior relationship. With a more favorable anterior overbite and overjet, the resorbed root of #9 would also have a better prognosis. The third image shows the pre-surgical decompensation that has been done by closing the spaces. (Fig. 3)
When I saw that patient, my thought was to retain the incisors and retract them thereby closing the edentulous canine sites and having the first premolars become the canines. Since the patient already required a Lefort procedure, why not advance the maxilla at the same time? This would allow the patient to keep his anterior teeth by correcting the anterior relationship. With a more favorable anterior overbite and overjet, the resorbed root of #9 would also have a better prognosis. The third image shows the pre-surgical decompensation that has been done by closing the spaces. (Fig. 3) The fourth image shows the patient post ortho/surgery. (Fig. 4) Note the significant improvement in tooth display compared to the initial. Radiographically the root of #9 hasn't changed appreciably, and following retention, the mobility has improved. The decision was made to retain #9 and, at the request of the patient, place veneers from canine to canine. The final restorations at 10 years post-treatment can be seen in the final image. (Fig. 5)
The fourth image shows the patient post ortho/surgery. (Fig. 4) Note the significant improvement in tooth display compared to the initial. Radiographically the root of #9 hasn't changed appreciably, and following retention, the mobility has improved. The decision was made to retain #9 and, at the request of the patient, place veneers from canine to canine. The final restorations at 10 years post-treatment can be seen in the final image. (Fig. 5) How long will the left central last? It's a difficult question to answer, but given that the treatment has lasted 10 years thus far with no changes, the likelihood is that it will continue proved a service. If it does ever require extraction and implant placement, just think how much better we are/will be with implants compared to where we were 10+ years ago.
How long will the left central last? It's a difficult question to answer, but given that the treatment has lasted 10 years thus far with no changes, the likelihood is that it will continue proved a service. If it does ever require extraction and implant placement, just think how much better we are/will be with implants compared to where we were 10+ years ago.Reference:
- Root resorption – Etiology, terminology and clinical manifestation. Tronstad L. Dental Traumatology 1988;4(6):241-52

Want to dive even deeper into clinical topics like this? Check out our clinical categories in our Course Library. Not yet a member of Spear Online? Click here to learn more.